
How to Reduce Alarm Fatigue in Nursing
Nurses on a busy hospital unit can face up to 1,000 alarms per shift, according to the American Association of Critical-Care Nurses. The vast majority of those alarms, between 85% and 99% by most estimates, do not require immediate action. The result is that monitor alarms lose their meaning. The alerts that matter compete for attention with hundreds that do not. Knowing how to reduce alarm fatigue in nursing is not about silencing alerts. The most effective alarm fatigue nursing interventions focus on process changes, not new technology. It is about restoring the meaning of each one.

- Alarm fatigue in nursing occurs when constant exposure to monitor alerts causes nurses to become desensitized, increasing the risk of delayed or missed responses to clinically significant alarms.
- A 2024 Academy of Medical-Surgical Nurses study confirmed that four nursing-led interventions on a 31-bed unit reduced total alarms by 40% and non-actionable alarms by 42.5% without replacing any monitoring equipment.
- The single most effective nursing intervention is per-patient alarm threshold customization at admission, shift change, and whenever a patient's clinical status changes.
- Charge nurses play a critical role in alarm fatigue reduction by establishing unit-level protocols, providing staff feedback, and ensuring threshold reviews are embedded in the standard handoff workflow.
- Clinical communication platforms that route alarm notifications directly to the responsible nurse's device reduce unit noise and improve response specificity without suppressing clinically important alerts.
- Alarm fatigue reduction requires ongoing oversight, not a one-time intervention. Units that establish quarterly data reviews and feedback loops sustain reductions over time.
Why Alarm Fatigue Hits Nurses Differently
Alarm fatigue hits nurses differently because nurses are the ones who hear every single alert in real time. Doctors and managers review alarm data in reports. Nurses live inside the noise: every alert, every patient, every shift.
The clinical consequence is well-documented. When most alarms do not need action, nurses start to tune them out. They delay responses, silence alerts without checking, or stop noticing abnormal readings. This is not poor nursing. It is a natural human response to constant noise. The fix is changing the environment, not blaming the nurse.

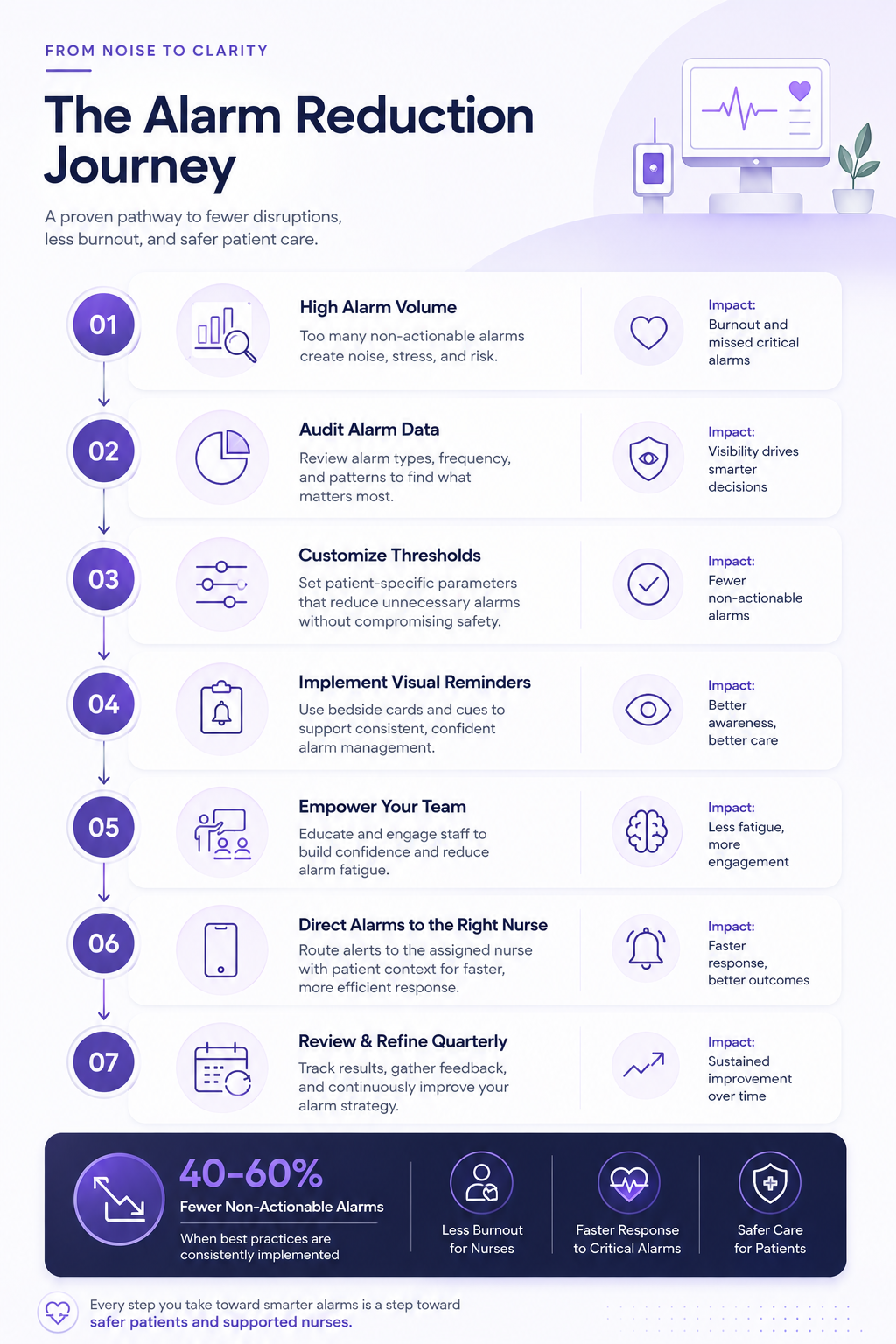
How to Reduce Alarm Fatigue in Nursing: A Step-by-Step Guide
Alarm fatigue in nursing can be reduced through six evidence-based steps: auditing alarm data, customizing thresholds per patient, adding visual cues, training the full care team, routing alerts to the right nurse, and reviewing data quarterly. None of these require new equipment, large budgets, or hospital-wide approval. A charge nurse can start the first three steps today.
Before changing anything, pull three to four weeks of alarm data from your monitoring system. Most systems have a built-in alarm history report. The goal is simple: find out which devices, alarm types, and times of day create the most unnecessary alerts on your unit.
This data gives you proof. You can show your unit director exactly which alarms dropped and by how much. Without a baseline, any improvement is just a feeling.
Default alarm settings are built for broad patient groups, not your specific patients. A patient with chronic atrial fibrillation does not need a heart rate alarm every few minutes. A patient on oxygen has a different safe SpO2 range than someone fresh out of surgery.
At each admission and shift handoff, the nurse should check and update the alarm settings for each patient. Settings should match that patient's current health status and documented baseline values. The AMSN 2024 unit study confirmed that this single intervention, combined with visual cues at the bedside prompting nurses to check parameters, produced a 42.5% reduction in non-actionable alarms on a 31-bed step-down unit within the study period.
Training alone is not enough to change habits in a busy unit. You also need visual reminders in the environment. The AMSN 2024 study used simple signs on doors and at the bedside to remind nurses to check alarm settings at admission and shift change. That combination worked better than training by itself.
A laminated card or sticker at each monitor asking "Have you checked alarm settings for this patient today?" takes minutes to make and costs nothing. It serves as a quick reminder during the moments most likely to be rushed: handoffs and new admissions.
Most alarm fatigue training is delivered to nurses only. But research from the Agency for Healthcare Research and Quality shows that programs covering the whole care team perform better. That includes doctors, respiratory therapists, and nursing assistants.
This matters because doctors sometimes set alarm parameters on admission orders without nurses reviewing them. A doctor who orders continuous monitoring without adjusting the settings creates a default alarm profile that fires unnecessary alerts for the whole stay. Training doctors too closes this gap at the source.
Training should cover three things: how to adjust alarm settings on your unit's monitors, what a clinically safe threshold looks like for your most common patient conditions, and how to document any changes in the patient chart.
Overhead alarms sound for the whole unit. Every nurse hears every alert, no matter whose patient triggered it. When an alarm fires, there is an unspoken question: whose job is it to respond? Under high workload, that question causes delays.
Clinical communication tools that connect to monitoring systems send each alert straight to the phone of the nurse responsible for that patient. The alert includes the patient name, room, and alarm type. This removes the guesswork, cuts down on noise, and creates a digital log of response times for future review.
Alarm fatigue improvements do not last on their own. Staff turns over. Patient complexity changes. New nurses join without the same training. Units that make early gains but do not review them regularly often see alarm rates creep back up within six months.
Establishing nursing alarm response protocols gives the whole team a shared set of rules, rather than relying on each nurse to decide on their own. A quarterly alarm review run by the charge nurse takes about 30 minutes. It answers three questions: Has total alarm volume gone up? Has the rate of unnecessary alarms changed? Are specific devices or times of day causing new spikes? The answers shape the plan for the next quarter.
Share this data with the full nursing team, not just management. When nurses see that their own threshold adjustments cut unnecessary alarms by 40%, they keep doing it because they can see it works.
What Charge Nurses Can Do Today
Charge nurses can reduce alarm fatigue starting this shift without waiting for policy changes or budget approval. Several of the highest-impact actions are within immediate nursing authority and take less than 10 minutes to initiate.
- Pull the alarm log for your unit from the monitoring system and identify the top 3 alarm categories by volume this week
- Add a threshold review reminder to today's shift handoff. Verbally prompt each incoming nurse to check parameters on their assigned patients before the outgoing nurse leaves
- Place a visual cue at one monitored bed as a pilot. A simple written prompt is sufficient to start
- Identify one physician on today's schedule who regularly orders continuous telemetry and have a brief conversation about individualized parameter defaults for their typical patient profile
- Set a calendar reminder for a 30-minute alarm data review at the end of this month
The Role of Communication Tools in Nursing Alarm Management
Clinical communication tools reduce alarm fatigue by routing each alert directly to the nurse responsible for that patient, cutting out the overhead noise that desensitizes the whole unit. Volume reduction and smart routing work together. Volume reduction and smart routing work together : neither alone solves the problem.

Even after cutting unnecessary alarms by 40%, the remaining alerts still need to reach the right nurse fast. Overhead systems that blast sound across the whole floor create confusion about who should respond. Alarm fatigue research consistently flags this coverage gap as a second major driver of the problem, separate from alarm volume.
When alarm notifications arrive on a nurse's personal device with the patient name, room number, and alert type included, the response decision is made faster, coverage responsibility is unambiguous, and the overhead noise environment improves for both patients and the rest of the care team. The acknowledgment record also gives charge nurses the data they need for Step 1 and Step 6 of this guide.
Evidence: A 2022 analysis published in the Journal of Hospital Medicine found that pager-dependent communication added an average of 4.7 minutes to emergency response times compared to real-time bidirectional messaging. In a cardiac arrest, 4.7 minutes matters enormously. The same is true for alarm response. The faster the right nurse is notified, the faster the response. And the quieter the unit environment becomes for everyone else.
Does Your Unit Have a Tool That Routes Alarms Directly to the Right Nurse?
HosTalky integrates with clinical alarm systems to deliver HIPAA-compliant notifications directly to the responsible nurse's device, with patient context included rather than just an alert sound.
See How HosTalky WorksFAQs
What is alarm fatigue in nursing and why does it matter?
How long does it take to see results from alarm fatigue interventions?
Can nurses adjust alarm thresholds on their own?
What is the difference between this article and alarm fatigue solutions for hospitals?
How do clinical communication platforms help with alarm fatigue?
Conclusion
Alarm fatigue in nursing is solvable. Units that commit to threshold customization, team education, visual cues, direct nurse routing, and quarterly reviews consistently see 40-60% alarm reductions. No new equipment needed. No hospital-wide project required. Just six steps, a charge nurse willing to lead them, and a review process to keep the gains in place. The evidence is clear. The only question is which shift you start.
Sources and References
- Nieve, M. (2024). Reducing Non-Actionable Alarms to Improve Patient Care and Staff Well-Being. Academy of Medical-Surgical Nurses. amsn.org
- The Joint Commission. (2025). National Patient Safety Goals: Clinical Alarm Safety. jointcommission.org
- American Association of Critical-Care Nurses. (2026). AACN Practice Alert: Alarm Management. aacn.org
- Sendelbach, S. and Drew, B. (2023). Reducing the Safety Hazards of Monitor Alert and Alarm Fatigue. Agency for Healthcare Research and Quality Patient Safety Network. psnet.ahrq.gov
- TigerConnect. (2026). Top 5 Strategies for Reducing Alarm Fatigue in Hospitals. tigerconnect.com
- Journal of Hospital Medicine. (2022). Pager vs. real-time messaging systems: emergency response time comparison.
